When your monthly prescription bill feels like a second rent payment, you’re not alone. In Australia, nearly one in five people skip doses or delay refills because they can’t afford their meds. And it’s not just about being tight on cash-it’s about staying healthy. The good news? There’s a proven way to cut your medication costs without giving up the treatment you need: asking for a therapeutic alternative.
What Is a Therapeutic Alternative?
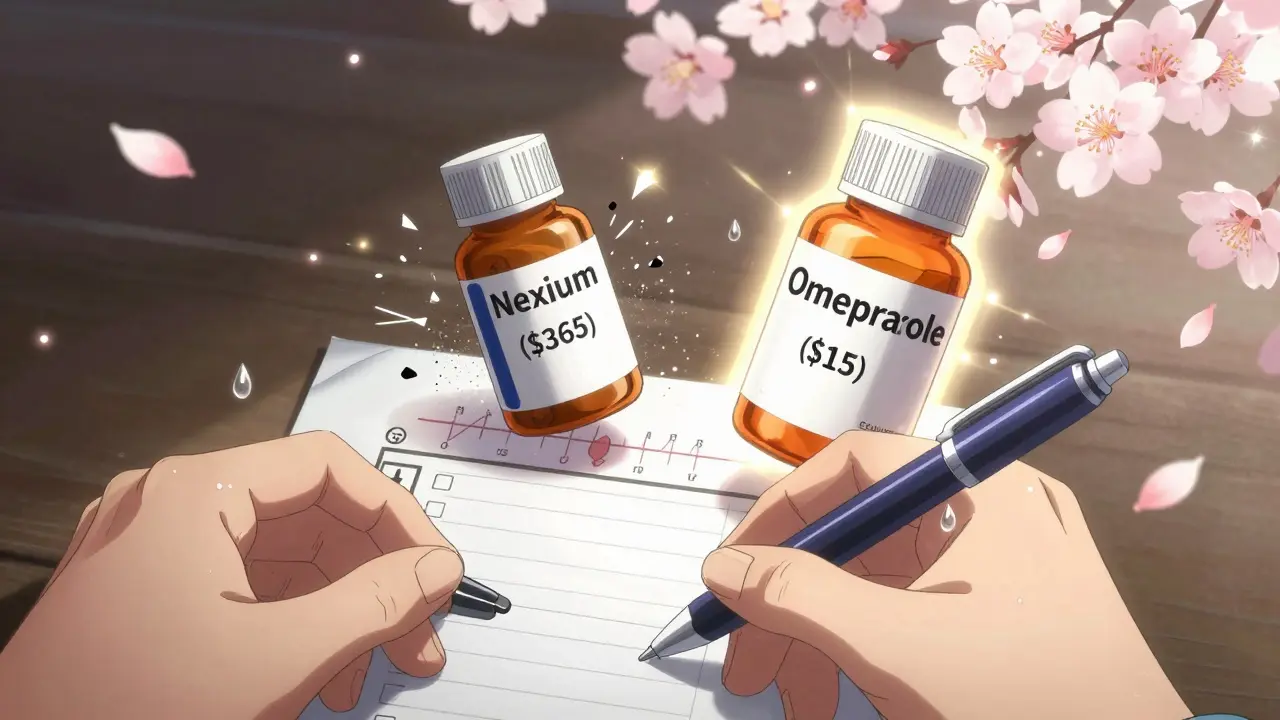
A therapeutic alternative isn’t just a cheaper version of your drug-it’s a different medicine that does the same job. Think of it like swapping one brand of painkiller for another. Both reduce fever, both ease headaches, but one might cost $10 instead of $80. For example, if you’re on esomeprazole (Nexium) for acid reflux, your doctor might suggest switching to omeprazole. Same class, same effect, but omeprazole costs about $15 a month instead of $365. That’s a 96% drop. Or if you’re on Eliquis for blood clots, warfarin might be an option-same protection, same monitoring, but a fraction of the price. This isn’t guesswork. It’s based on decades of clinical research showing these alternatives work just as well for most people. The key difference? Therapeutic alternatives are chemically different drugs from the same category. Generic substitution means you get the exact same chemical, just cheaper. Therapeutic interchange means you get a different chemical that acts the same way.Why Doctors Don’t Always Suggest It
You might wonder why your doctor hasn’t brought this up. The truth? Many don’t know the full range of options. Or they’re worried about side effects. Or they assume you’re fine with the cost. A 2023 survey found that 37% of patients had trouble convincing their doctor to consider a cheaper alternative. Some doctors fear patients will have worse outcomes-even though studies show no difference in hospital visits or disease control when switching to a proven alternative. The bigger issue? Time. A typical GP visit is 10 minutes. Asking about cost isn’t always part of the script. But it should be. The American Academy of Family Physicians recommends starting every visit with one simple question: “Do you ever have trouble affording your medications?” If you say yes, the conversation should shift to solutions.How to Ask for a Therapeutic Alternative
Here’s how to make the request-clear, confident, and backed by facts.- Know your drug and its class. Look up your medication online. Is it a statin? A beta-blocker? A PPI? Knowing the class helps you ask the right questions. For example: “I’m on atorvastatin for cholesterol. Are there other statins that work the same but cost less?”
- Check prices yourself. Use tools like GoodRx or your local pharmacy’s price list. Many chains (Woolworths, Chemist Warehouse, Pharmacy Direct) offer $5-$10 lists for common generics. Print or screenshot the prices. Show your doctor: “This version costs $12. Can we try it?”
- Be specific. Don’t say, “Can I get something cheaper?” Say, “Can I switch from lisinopril to benazepril? I read they’re equally effective for blood pressure.”
- Ask about patient assistance programs. Many drug makers offer free or low-cost meds if you qualify. Sites like NeedyMeds and RxAssist list programs by drug name. Some even cover brand-name drugs for under $10 a month.
- Request a 90-day supply. If your insurance allows it, asking for a 3-month supply can cut your copay by 25%. It’s easier to manage, and you’re less likely to run out.
When It Works Best
Therapeutic alternatives shine in chronic conditions where you take the same drug every day:- High blood pressure (lisinopril, amlodipine, hydrochlorothiazide)
- Diabetes (metformin, glimepiride, sitagliptin)
- Cholesterol (atorvastatin, simvastatin, rosuvastatin)
- Acid reflux (omeprazole, pantoprazole, ranitidine)
- Depression and anxiety (sertraline, citalopram, fluoxetine)
When It Doesn’t Work
Not every drug has a safe alternative. This is especially true for:- Cancer treatments
- Autoimmune drugs like biologics (Humira, Enbrel)
- Seizure medications
- Some mental health drugs
What to Do If Your Doctor Says No
If your doctor refuses, don’t walk away. Ask for more info:- “Is there a reason you don’t think this alternative would work for me?”
- “Can we try a small trial dose to see how I respond?”
- “Is there a formulary exception I can apply for?”
Real Stories, Real Savings
One man in Melbourne switched from brand-name Lyrica to generic gabapentin for nerve pain. His monthly cost dropped from $450 to $15. He started taking it regularly for the first time in years. A woman in Sydney changed from Eliquis to warfarin. Her copay went from $450/month to $18. She had to get blood tests every few weeks, but she could afford her meds again. Another patient switched from Crestor to atorvastatin. Saved $380 a month. No change in cholesterol levels. No side effects. These aren’t rare cases. A 2024 survey of 12,500 patients found that 68% successfully got a cheaper alternative through their doctor. Average monthly savings? $47.25. That’s over $500 a year-enough to cover a dental check-up, a new pair of glasses, or a month’s worth of groceries.What’s Changing in 2026
New tools are making therapeutic interchange easier. Electronic health systems now flag possible swaps at the moment your doctor clicks “prescribe.” Some apps even show real-time pharmacy prices. In Australia, the PBS (Pharmaceutical Benefits Scheme) is expanding its list of low-cost alternatives. More drugs are being reviewed for cost-effectiveness. And patient advocacy groups are pushing for clearer guidelines so doctors feel confident making these switches. The goal isn’t to cut corners. It’s to make sure you can keep taking your medicine-without going broke.Final Checklist: Your Action Plan
Before your next appointment, do this:- Write down every medication you take, including dose and frequency.
- Check the price of each at your local pharmacy. Use the PBS website or GoodRx.
- Identify which ones cost more than $50/month.
- Look up their therapeutic class (Google “[drug name] drug class”).
- Find one cheaper alternative in that class.
- Write down the name of the alternative and its price.
- At your appointment, say: “I’ve been struggling with the cost of [current drug]. I found [alternative] costs much less. Can we talk about switching?”
Frequently Asked Questions
Is a therapeutic alternative the same as a generic drug?
No. A generic drug is the exact same chemical as the brand-name version-just cheaper. A therapeutic alternative is a different chemical that works in the same way. For example, lisinopril and benazepril are both ACE inhibitors for high blood pressure, but they’re not the same molecule. Generics are usually cheaper, but therapeutic alternatives open up more options when no generic exists.
Can I switch to a therapeutic alternative on my own?
No. Never switch medications without talking to your doctor or pharmacist. Even if two drugs seem similar, they can affect your body differently. Some cause side effects others don’t. Others interact with other meds you’re taking. Your doctor needs to approve any change.
Will my insurance cover a therapeutic alternative?
Usually, yes. Most insurance plans (including Medicare and private insurers) prefer lower-cost alternatives. If your current drug is on a higher tier, your doctor can request a tier exception. Many plans have a fast-track process for cost-related exceptions.
How long does it take to get a therapeutic alternative approved?
If your doctor writes the prescription and it’s on your plan’s formulary, you can pick it up the same day. If a prior authorization is needed, it can take 2-7 days. For urgent cases, many insurers will approve it within 72 hours if your doctor explains why the original drug is unaffordable.
What if the alternative doesn’t work for me?
That’s why you start with a trial. Your doctor will likely suggest trying the new drug for 4-6 weeks. If your symptoms return or side effects appear, you can switch back. Most plans allow you to go back to your original medication without penalty if it’s medically necessary.
Are there free programs to help pay for medications?
Yes. Programs like NeedyMeds, RxAssist, and the PBS Safety Net can help. Some drug manufacturers offer free or discounted meds if your income is below a certain level. Pharmacists can help you apply. Don’t assume you don’t qualify-many people do.


Akshaya Gandra _ Student - EastCaryMS
January 4, 2026 AT 22:01so i read this and was like wait can i do this for my metformin? my doc never mentioned cheaper options and i’ve been paying $70/month… this changed my whole perspective
John Wilmerding
January 5, 2026 AT 10:41This is an exceptionally well-researched and clinically grounded guide. I appreciate how you distinguished therapeutic interchange from generic substitution-a nuance often overlooked even by healthcare professionals. The inclusion of real-world cost comparisons and actionable steps empowers patients to advocate for themselves with evidence, not just emotion. Pharmacists, in particular, are underutilized allies in this process; their training in pharmacokinetics and formulary knowledge makes them ideal collaborators in cost-reduction strategies. I urge all clinicians to integrate affordability screenings into routine care, as recommended by the AAFP. This isn’t charity-it’s competent, ethical medicine.
Peyton Feuer
January 6, 2026 AT 04:08my doctor laughed when i asked about switching from Eliquis to warfarin… said i’d ‘be lucky not to bleed out.’ but i did my homework, showed him the studies, and now i’m on it. blood tests? yeah. but i saved $400/month. worth it.
Siobhan Goggin
January 6, 2026 AT 11:00I wish more people knew about this. It’s not about cutting corners-it’s about not having to choose between health and rent. Thank you for writing this.
Cassie Tynan
January 7, 2026 AT 18:39Oh wow, so now we’re supposed to be medical detectives just to afford our prescriptions? How quaint. Let me guess-next they’ll ask us to diagnose ourselves with a Google search and a Ouija board.
melissa cucic
January 8, 2026 AT 02:41It is, indeed, a profoundly ethical imperative that patients be empowered with information regarding therapeutic alternatives; yet, the systemic failure to integrate cost-awareness into clinical practice remains a moral lacuna. The physician-patient relationship ought to be one of shared inquiry-not paternalistic assumption. That 37% statistic is not merely a number; it is a testament to institutional neglect. One must ask: if a drug is clinically equivalent, why is affordability not a primary criterion in prescribing? The answer, I fear, lies not in medicine, but in market forces that prioritize profit over personhood.
Jay Tejada
January 9, 2026 AT 18:36bro i switched from lyrica to gabapentin last year… same pain relief, $12 instead of $450. my doctor was like ‘uh… sure?’ like he’d never heard of it. i think he thought i was trying to scam the system. but i just wanted to not be broke every month.
Allen Ye
January 11, 2026 AT 17:00Let me tell you something about the American healthcare system: it doesn’t care if you live or die-it cares if you can pay for the paperwork to prove you’re sick. This post isn’t just about drugs-it’s about the quiet, daily violence of medical capitalism. We’ve turned healing into a transaction where the price tag is a verdict. The fact that a man in Melbourne can save $435/month by switching from Lyrica to gabapentin isn’t a win-it’s a scandal. And yet, here we are, celebrating it like it’s a discount coupon. We’ve normalized exploitation. We’ve turned medical necessity into a bargaining chip. And the people who suffer? They’re not ‘patients.’ They’re ‘cost centers.’ Until we treat healthcare as a human right-not a luxury reserved for those who can afford the fine print-we’re not fixing anything. We’re just rearranging deck chairs on the Titanic.
mark etang
January 12, 2026 AT 04:45It is imperative to acknowledge the clinical efficacy and cost-effectiveness of therapeutic interchange as a validated strategy within evidence-based practice. The data presented herein aligns with established guidelines from the American College of Physicians and the American Heart Association. Furthermore, the utilization of formulary resources and patient assistance programs constitutes a responsible and proactive approach to pharmaceutical management. I commend the author for providing a structured, actionable framework that facilitates patient-centered decision-making without compromising therapeutic outcomes.
josh plum
January 14, 2026 AT 02:12Of course the pharma companies don’t want you to know this. That’s why your doctor doesn’t mention it-they’re paid by Big Pharma to keep you on the expensive stuff. They’re not your doctor-they’re a sales rep in a white coat. And the FDA? They’re in the tank too. Just wait, soon they’ll start charging you to breathe. This isn’t about medicine. It’s about control.
Ashley Viñas
January 14, 2026 AT 04:06I’m so tired of people treating healthcare like a budgeting spreadsheet. Not every drug has a ‘cheaper version.’ Some people need the real thing. If you’re too lazy to pay $50 a month for your meds, maybe you shouldn’t be on them at all. This post is dangerously naive. Medicine isn’t Amazon. You can’t just swap out ingredients and hope for the best. Some of us have lives on the line-not discount codes.
Aaron Mercado
January 16, 2026 AT 03:54You people are ridiculous. You think swapping drugs is some kind of ‘hack’? You’re playing Russian roulette with your health. My cousin switched to a ‘cheaper’ antidepressant and ended up in the psych ward. Now he’s on disability. And you’re all patting yourselves on the back like you’re heroes? You’re not saving money-you’re gambling with your brain. And for what? A few bucks a month? You’re not frugal-you’re reckless. And you’re putting other people at risk by normalizing this nonsense.